


Targeted Therapies for Inflammatory Bowel Disease (IBD)
By Tingxu Chen
May 28, 2025



Inflammatory bowel disease (IBD) is a chronic, relapsing condition of the gastrointestinal tract, primarily encompassing ulcerative colitis and Crohn's disease (CD). Ulcerative colitis (UC) is confined to the colonic mucosa and typically presents with continuous inflammation. CD, on the other hand, can affect the entire gastrointestinal tract, especially the terminal ileum and colon, with transmural and segmental lesions that often cause abdominal pain, intestinal strictures, or fistula formation, significantly impairing patients' quality of life (Figure 1). Recent studies investigating the inflammatory target TSLP have also highlighted the role of epithelial-derived cytokines in regulating mucosal immunity and chronic intestinal inflammation associated with IBD.
Common IBD symptoms include abdominal pain, diarrhea, rectal bleeding, fatigue, and weight loss. In severe IBD, complications such as Fistulizing Crohn's disease and extraintestinal manifestations substantially increase disease burden and healthcare utilization.
From 1990 to 2021, global IBD incidence increased by over 88%, with projections exceeding 20 million affected individuals by 2040. This growing prevalence highlights the urgent need for effective treatment strategies that address both symptom control and disease modification. Moreover, there is a growing trend of younger individuals being diagnosed with IBD each year [3].
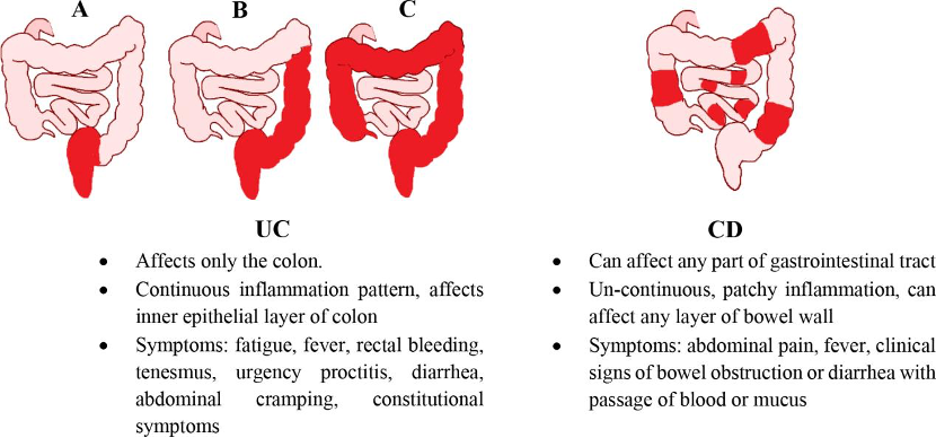
Figure 1. Classification and Main Clinical Features of Inflammatory Bowel Disease (IBD) [1] (A. Proctitis; B. Left-sided colitis; C. Extensive colitis. Differences between UC and CD)
From 1990 to 2021, the global incidence of IBD has increased by 88.30%, reaching 375,140 cases. It is projected that by 2040, the global IBD patient population will exceed 20 million, making it a newly emerging global public health crisis. Moreover, there is a growing trend of younger individuals being diagnosed with IBD each year [3].
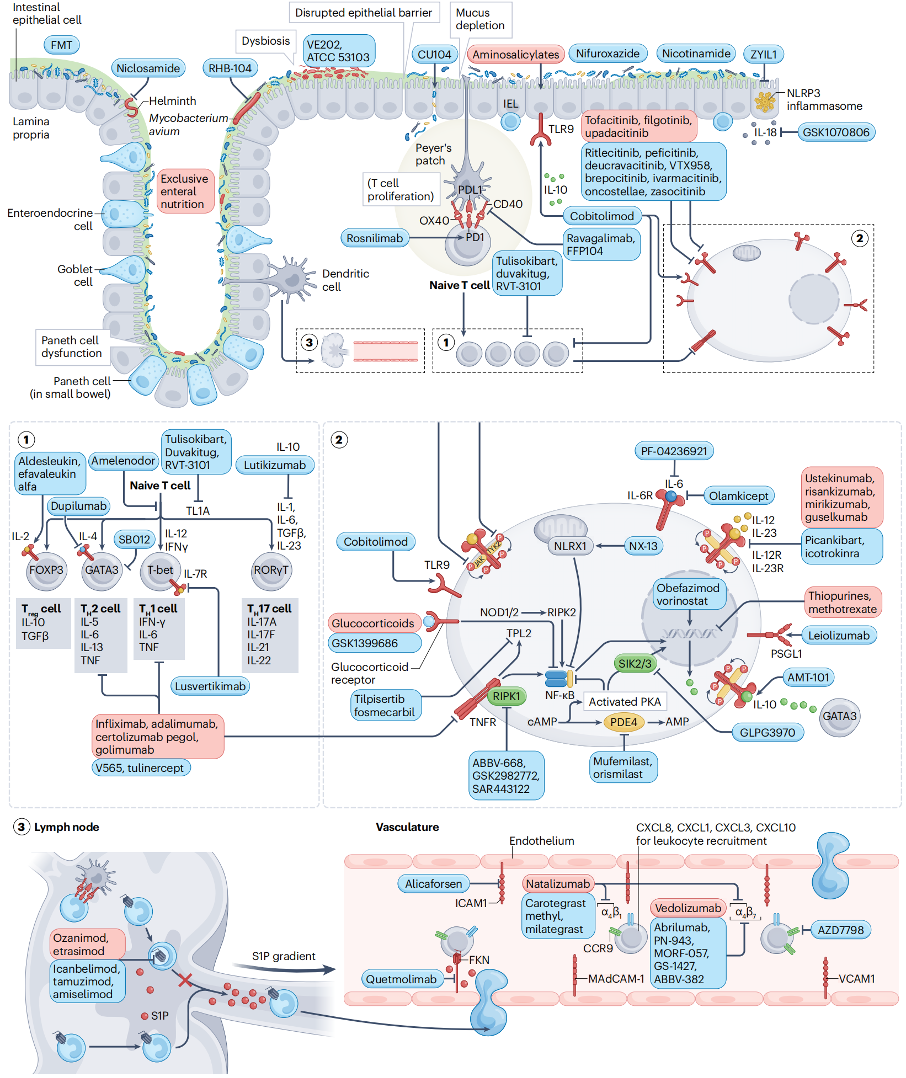
Pathogenesis and Immune Dysregulation in IBD
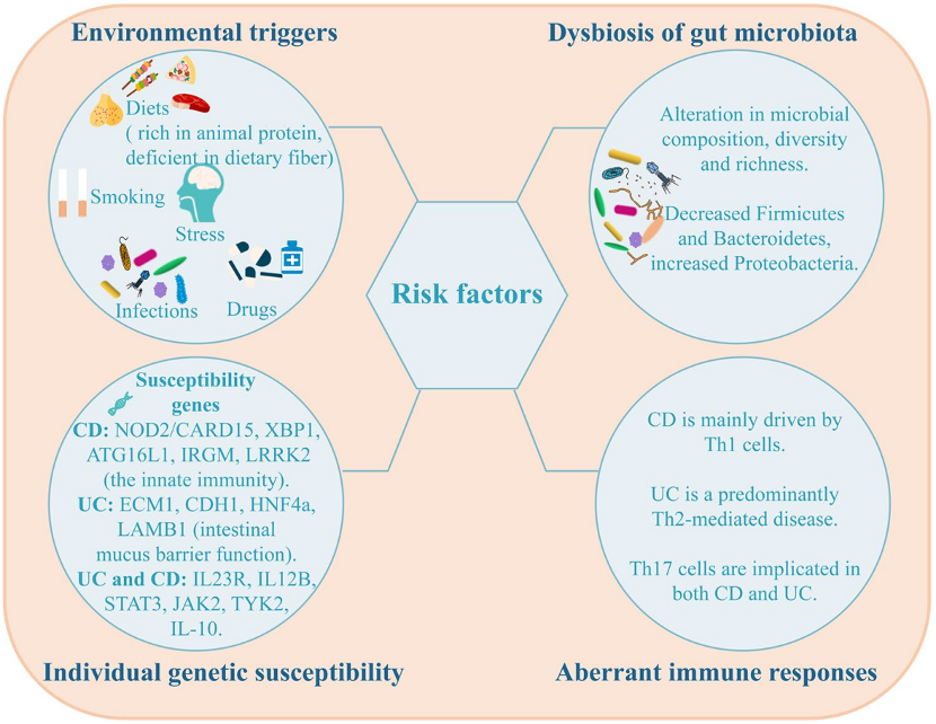
IBD arises from a complex interplay of genetic risk factors. Genetic mutations increase susceptibility, while immune system dysregulation triggers inflammatory attacks on healthy gut tissue. Imbalances in the gut microbiota and external factors such as a poor diet or infections can further disrupt intestinal homeostasis.
Key processes include:
-
Dysregulated cytokine signaling
-
Impaired epithelial barrier function
-
Altered lymphocyte trafficking via lymph nodes
-
Microbiota-driven immune activation
These mechanisms vary by disease type, contributing to heterogeneous responses to IBD treatment and explaining why many patients fail to respond to first-line therapies.
These overlapping causes lead to wide variability in symptoms, disease course, and treatment response. Most patients need long-term therapy, with frequent relapses, especially in Crohn’s, where recurrence exceeds 60%. With no cure yet, there remains a substantial need for improved treatments.
Current Landscape of Targeted Therapies for IBD
Conventional IBD treatments (e.g., aminosalicylates, corticosteroids) offer symptom relief but fall short in long-term efficacy and safety. As a result, biologics and other newer therapies now form the backbone of care for moderate-to-severe and severe disease.
1. Inflammatory Response Control
Key therapeutic targets include:
→ Tumor Necrosis Factor-alpha (TNFα): Rapid Inflammation Control
TNFα and IL-12/IL-23 inhibitors marked major advances in IBD treatment, helping control symptoms and inflammation. While anti-TNF agent drugs like Adalimumab and Ustekinumab remain common, their effectiveness can be limited by resistance and safety issues. Newer therapies are now targeting alternative inflammatory pathways.
→ IL-12, IL-23, and Their Receptors: Reduction of Chronic Gut Inflammation
Inflammation
-
Ustekinumab: Targets the shared p40 subunit; approved for UC/CD since 2009.
-
Guselkumab: Selective IL-23 p19 blocker; approved in 2025 for Crohn’s.
-
Other IL-23p19 inhibitors: Include Risankizumab (AbbVie, 2019) and Mirikizumab (Eli Lilly, 2023).
→ Emerging Targets: TL1A and OSMRβ
TL1A is a TNF-like cytokine that activates DR3 to drive inflammation and fibrosis via Th17 cells, cytokine release, and fibroblast activation.
OSMRβ, expressed in intestinal stromal cells, contributes to fibrosis and chronic inflammation. Targeting this pathway may benefit patients with severe IBD who do not respond to existing biologic drug classes.
Both forms are active; the soluble form may serve as a biomarker.
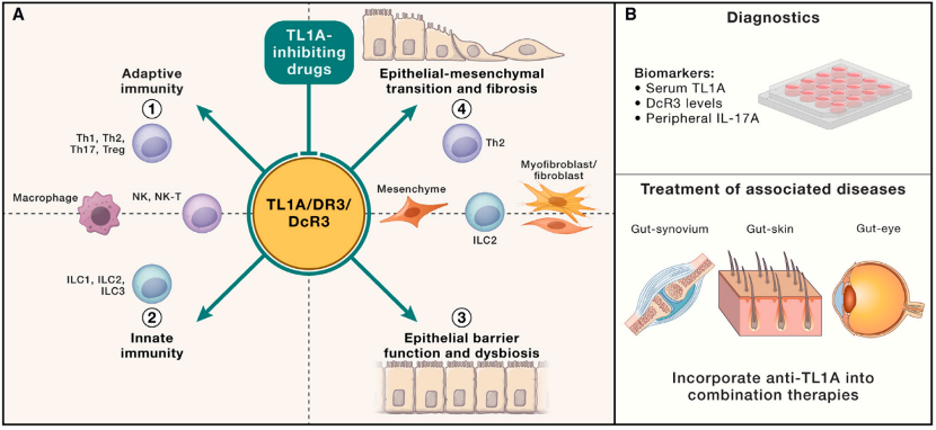
Targeting TL1A offers a dual approach by reducing both inflammation and fibrosis, positioning it as a potential disease-modifying therapy for IBD. With gaps in current treatment efficacy, TL1A is gaining momentum as a promising, safe option that’s attracting significant interest from global pharmaceutical companies.
Although no TL1A-targeted drugs are approved yet, 2023 marked significant momentum:
- Merck acquired Prometheus Biosciences for $10.8 billion, securing the TL1A antibody Tulisokibart (PRA-023 / MK-7240)—the largest autoimmune M&A to date.
- Sanofi licensed Duvakitug (TEV574) from Teva for $1.5 billion.
- Roche bought Telavant from Roivant for $7.1 billion, obtaining rights to PF-06480605 (now RG-6631 / RVT-3101), originally developed by Pfizer.
Clinical results have highlighted TL1A antibodies as top candidates for IBD. In 2024, AbbVie licensed FG-M701 from Mingji Biopharma for $1.7B.
OSMRβ, found in gut stromal cells, drives inflammation and fibrosis via OSM and IL-31 signaling. Vixarelimab, an anti-OSMRβ antibody from Roche and Genentech, is in Phase II trials for ulcerative colitis.
2. Inhibiting Immune Cell Adhesion and Migration
Representative targets: Integrin α4β7, MAdCAM-1
This approach aims to block the interaction between integrins and their ligands on vascular endothelial cells, thereby preventing lymphocytes from crossing the endothelium and migrating to inflamed sites.
- Vedolizumab blocks α4β7 from binding to MAdCAM-1 without affecting α4β1–VCAM-1 interactions thereby preserving CNS immune surveillance and reducing the risk of PML. It’s especially suited for patients unresponsive to conventional or anti-TNFα therapies.
- Ontamalimab (SHP64), a MAdCAM-1 inhibitor from Pfizer later acquired by Takeda, was discontinued due to the absence of a licensing partner.
3. Promoting Tissue Repair
Key target: TGF-β (Transforming Growth Factor Beta)
TGF-β is a multifunctional cytokine that promotes M2 macrophage differentiation, dampens inflammation, and supports tissue repair by inducing ECM synthesis.
A key product in this space is Modulen, a TGF-β2-enriched nutritional formula launched in China in February 2025. With good taste and broad use, it's especially suited for pediatric patients.
The progression of biologic targets in IBD—from early TNFα inhibitors to integrins, interleukins, and now novel targets like TL1A—highlights a strategic shift from symptom control to precision and full immune modulation. Treatment choice depends on disease type, patient tolerance, and individual needs, with combination therapies sometimes required.
Below is a summary of approved and investigational targeted therapies for Ulcerative Colitis (UC) and Crohn’s Disease (CD):
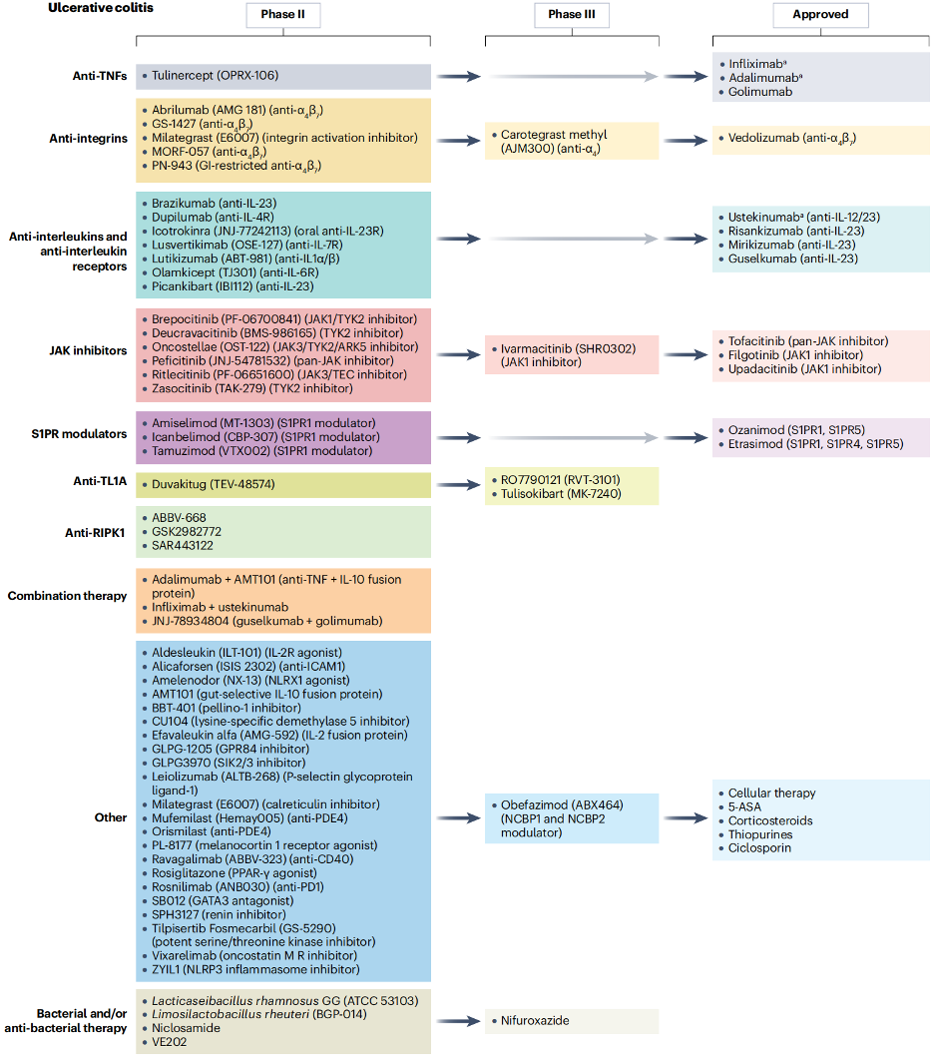
Figure 5. Approved and Investigational Targeted Therapies for Ulcerative Colitis (UC) [6]
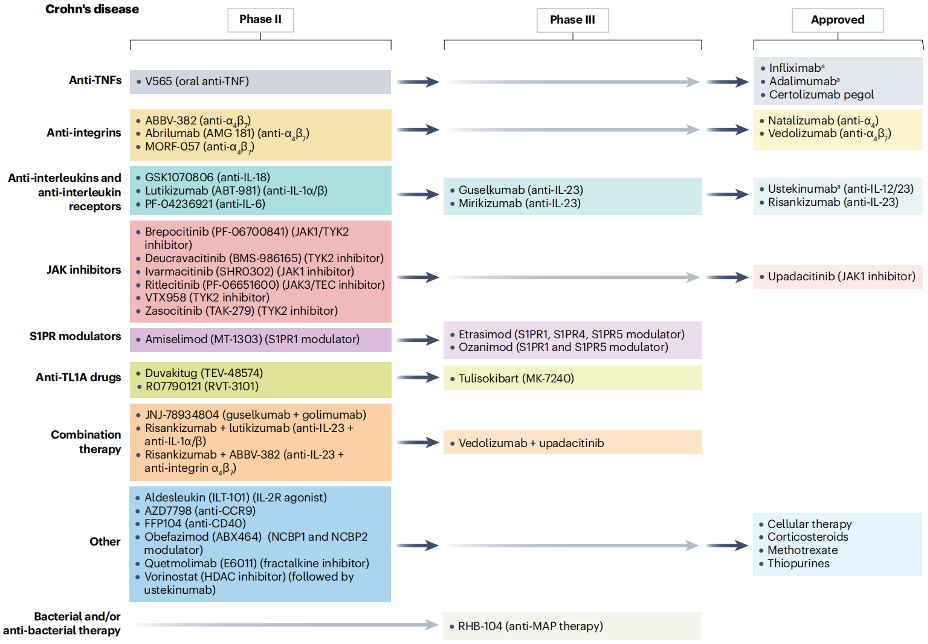
Figure 6. Approved and Investigational Targeted Therapies for Crohn’s Disease (CD) [6]
KACTUS Solutions for IBD Research
The growing demand for new drugs for IBD treatments is driving continuous expansion of the related pharmaceutical market, and each innovative therapy brings new hope to patients. KACTUS offers a wide range of high-quality recombinant proteins essential for IBD drug development. These products cover key targets such as TNFα, IL-23, TL1A, integrins, and more—supporting research needs across all stages of development. For projects requiring affinity analysis or kinetic characterization of antibody-target interactions, our SPR services offer precise, real-time binding data to accelerate development timelines.
Example Data:
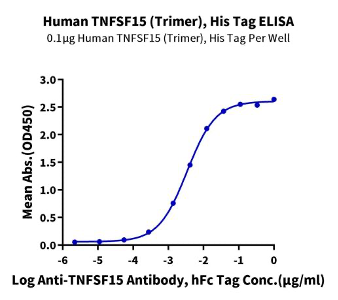
Immobilized Human TNFSF15 Trimer, His Tag at 1 μg/ml (100 μl/Well) on the plate. Dose response curve for Anti-TNFSF15 Antibody, hFc Tag with the EC50 of 3.4 ng/ml determined by ELISA (QC test).
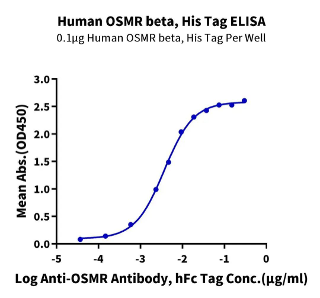
Immobilized Human OSMR beta, His Tag at 1 μg/ml (100 μl/Well) on the plate. Dose response curve for Anti-OSMR Antibody, hFc Tag with the EC50 of 3.7 ng/ml determined by ELISA (QC Test).
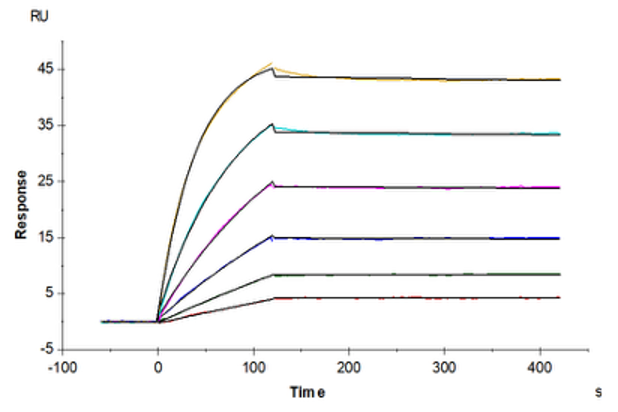
Human DR3, hFc Tag captured on CM5 Chip via Protein A can bind Human TNFSF15 Trimer, His Tag with an affinity constant of 0.10 nM as determined in SPR assay (QC test).
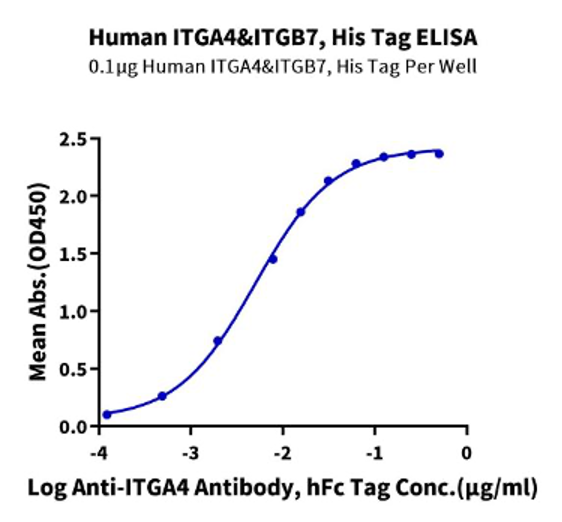
Immobilized Human ITGA4&ITGB7, His Tag at 1 μg/ml (100 μl/well) on the plate. Dose response curve for Anti-ITGA4 Antibody, hFc Tag with the EC50 of 5.0 ng/ml determined by ELISA (QC Test).
FAQs: Targeted Therapies for Inflammatory Bowel Disease
1. What distinguishes targeted therapies from conventional IBD medications?
Targeted therapies for inflammatory bowel disease selectively inhibit immune pathways that drive disease rather than broadly suppress immunity. Compared with conventional therapy, biologics improve specificity, reduce off-target toxicity, and increase the likelihood of endoscopic remission and mucosal healing.
2. Why do some IBD patients lose response to anti-TNF agents?
Loss of response to anti-TNF therapy can result from immunogenicity, pharmacokinetic variability, or the emergence of alternative inflammatory pathways. This explains why many patients require newer therapies or combination strategies over time.
3. How is remission defined in modern IBD treatment?
Modern goals extend beyond symptom control to include clinical remission, endoscopic remission, and biomarker normalization. Achieving deep remission correlates with reduced hospitalization, surgery, and disease progression.
4. What role do biomarkers play in treatment decisions?
Markers such as fecal calprotectin provide a noninvasive assessment of intestinal inflammation and correlate with endoscopic response. Biomarker-guided management improves treatment precision and reduces unnecessary exposure to ineffective drugs.
5. How do emerging targets like TL1A change the treatment landscape?
TL1A-targeted therapies aim to modify disease biology rather than solely suppress inflammation. Early data suggesting durable clinical response and fibrosis control indicate potential for improved long-term efficacy, particularly in severe IBD.

60 Hickory Drive
Waltham, MA 02451
United States
Targeted Therapies for Inflammatory Bowel Disease (IBD)