


Expanding Landscape of TCR Therapies: Clinical Breakthroughs, Formats, and Production Support
By Tingxu Chen
June 12, 2025
Featured Products






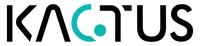
At the 2023 ISCT conference, SCG Cell Therapy announced breakthrough clinical data for its autologous TCR-T cell injection SCG101 in the treatment of HBsAg-positive liver cancer—a milestone underscoring the growing role of advanced proteins and enzymes for cell therapy in enabling next-generation immunotherapies. The partial response (PR) rate reached 66%, with one lesion further shrinking by 74.5% by month 4 and another lesion disappearing completely. These promising clinical trial results demonstrate the therapeutic potential of HBsAg-targeted TCR-T therapy and mark a significant milestone for T cell therapies in solid tumors. In recent years, TCR therapies have emerged rapidly, achieving continuous clinical breakthroughs and gradually becoming a rising force in the field of immunotherapy. As a cancer immunotherapy approach, TCR therapy is designed to help the body’s immune system recognize and destroy cancer cells, particularly in treating solid tumors where conventional options may be limited. This positioning is especially relevant for treating solid tumors, especially solid tumors with limited actionable cell surface targets.
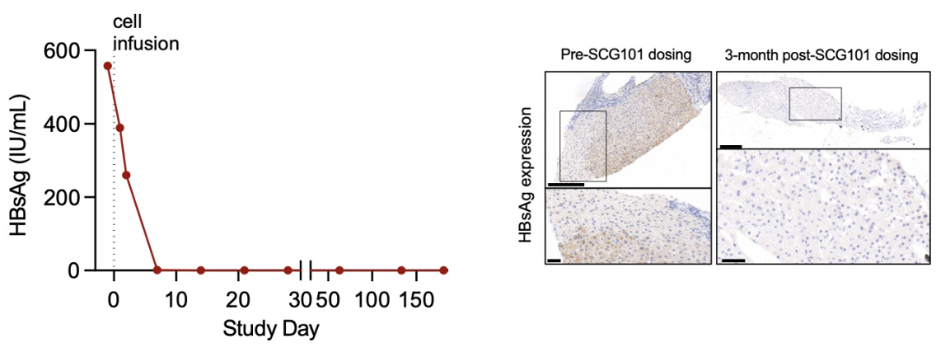
Figure 1. Selected Clinical Data of SCG101 [1].
TCR Therapy
TCR therapy is a novel form of immunotherapy developed based on the natural recognition pattern between T cell receptors (TCRs) and antigens. Therapeutic formats include adoptive T cell therapy (TCR-T) and TCR-based protein drugs (such as TCR-scFv and TCR mimic antibodies). In simple terms, the T cell receptor is one of the key cell receptors that guides antigen recognition and downstream cell responses in immune cells. This linkage between cell receptors and the immune system helps direct T cells toward tumor cells while minimizing activity against healthy cells. T cells are the body’s immune lymphocytes that execute this antigen-guided targeting.
TCR-T works by first screening and validating TCR sequences that can recognize specific antigens. These sequences are then genetically engineered into a patient’s T cells, enabling the modified T cells to specifically bind to and kill tumor cells expressing the target antigen. This TCR-T cell therapy relies on genetically engineered / genetically modified and often engineered T cell products, including engineered T cell receptors created from a defined TCR sequence, with functional tuning influenced by the TCR chain and the underlying TCR gene.
In some development workflows, gene editing is used alongside genetic engineering to optimize engineered T cells while maintaining safety controls. In this context, the “antigen” refers to a complex formed by intracellular antigenic peptides presented on MHC (or HLA) molecules at the cell surface. These peptide fragments can originate from abnormal proteins generated inside cancerous cells, meaning TCR therapies can access intracellular proteins rather than being limited to cell surface antigens.
The structural diversity of MHC complexes and their peptide-binding profiles play a critical role in shaping the specificity and efficacy of TCR recognition. Precise control over the design and composition of MHC monomers and tetramers can significantly impact the reliability of downstream immunological assays and therapeutic validations. Utilizing an MHC complex custom service allows researchers to tailor these complexes to match unique antigenic contexts, thereby improving the fidelity of TCR-antigen interaction studies.
Through this unique recognition mechanism, TCR-T can target a broader range of intracellular antigens and has shown particularly promising results in the treatment of solid tumors. In practice, these target antigens / tumor antigens are evaluated for safety against healthy cells, normal cells, and normal tissues to reduce cross reactivity and unintended damage. The binding affinity and specificity of such TCR-antigen interactions can be quantitatively assessed using techniques like our surface plasmon resonance service, which supports precision in TCR candidate evaluation. This strengthens T cell therapies by improving how antigen recognition is measured for each TCR T cell candidate. This includes confirming whether a candidate TCR maintains high affinity without increasing off-target risk.
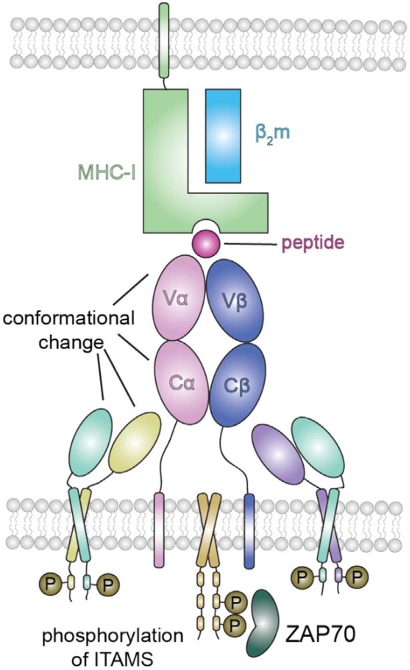
Figure 2. TCR recognizes MHC-peptide complex [2].
High specificity and sensitivity are defining features of TCR-T therapy. It can elicit strong T cell responses even against low-density antigen populations, while also carrying a lower risk of cytokine release syndrome. Additionally, compared to CARs, TCRs typically have lower affinity and faster dissociation rates, allowing for repeated antigen recognition and signal triggering, which helps amplify immune responses. This distinction matters when comparing TCR-T with chimeric antigen receptor platforms, which more commonly recognize cell surface antigens directly on tumor cells. In that comparison, chimeric antigen receptor approaches can be highly effective, but they differ from T cell receptor therapies in how cell receptors engage tumor cells.
Figure 3. TCR-T treatment process [3].
TCR-scFv and TCR mimic antibodies represent a new class of protein engineering technologies that develop protein-based therapeutics centered on TCR or TCR-like structures, without the need for gene engineering or adoptive cell transfer. In these applications, the precise expression of custom protein formats, such as engineered TCR components, may benefit from custom protein expression services to ensure structural accuracy and functional performance. Here, reliable TCR expression supports consistent activity across cells and reduces variability during development. This simplifies the manufacturing process and offers a more streamlined treatment option for clinical use. A representative drug is Tebentafusp (brand name Kimmtrak), currently the only approved TCR-based therapy on the market. It simultaneously targets the GP100 peptide–HLA*02:01 complex and CD3. This mechanism helps T cells focus on cancer cells while supporting efforts to fight cancer with controlled immune-cell engagement.
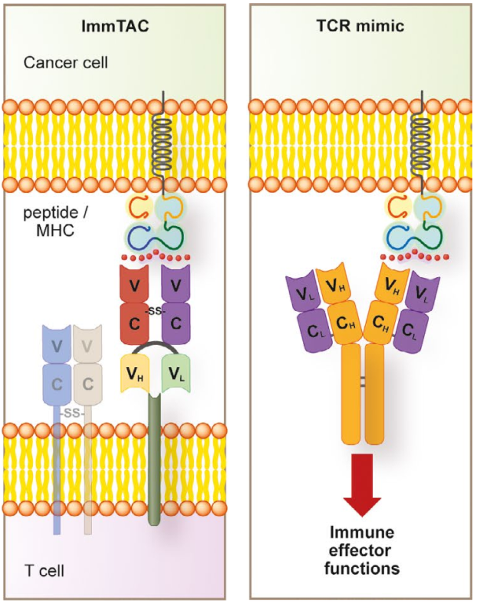
Figure 4. TCR-like structure [4].
Progress in TCR Therapies
Tebentafusp has shown strong market momentum, generating $55.09 million in revenue in Q1 2023. More importantly, it has significantly extended patient survival and has become the most prescribed drug for HLA*02:01-positive metastatic uveal melanoma. This is often discussed alongside broader metastatic melanoma needs in melanoma patients, reinforcing the role of T cell receptor therapies within modern cancer care. In the U.S., several companies are actively advancing TCR therapies, including TCR² Therapeutics, Lyell Immunopharma, Intellia Therapeutics, and Kite Pharma, with multiple clinical-stage candidates already in development. These clinical trials aim to extend TCR therapy into additional solid tumors by directing immune cells to eliminate cancer cells and tumor cells more selectively.
Outside the U.S., companies such as Adaptimmune (UK), Immunocore (UK), Medigene (Germany), and RootPath (China/U.S.) are also driving innovation in TCR therapeutics. In 2024, FDA has granted accelerated approval to afamitresgene autoleucel (commercial name ‘Tecelra’, Adaptimmune) for unresectable or metastatic synovial sarcoma. This metastatic synovial sarcoma milestone supports the growing role of cellular therapy / cell therapy as a cancer treatment and cancer therapy option in immuno-oncology.
Other clinical-stage pipelines include MDG1011(Medigene), lete-cel (Adaptimmune). In 2023, Adaptimmune and TCR² have announced a strategic merger [5], forming a new company that integrates both SPEAR and TRuC platforms to enable recognition of both intracellular and extracellular targets. Strategically, these formats aim to broaden more targets while maintaining safety.
Across these pipelines, T cell therapy is designed to improve outcomes for patients with solid tumors by pairing antigen-specific recognition with careful protection of healthy cells. TCR therapy brings renewed hope to the field of immunotherapy for solid tumors, with broad and promising clinical potential. However, it also faces significant challenges, such as the isolation and purification of T cells in TCR-T therapy, the identification of safer and more specific targets, and the need for appropriate HLA matching. These limitations may hinder the development of off-the-shelf TCR-T products, thus affecting accessibility. Key translational considerations include ensuring antigen presenting cells support the intended immune response, managing T cell activity within the tumor microenvironment, and confirming that targeting does not harm normal tissues. Nevertheless, these challenges have sparked new avenues of exploration, such as γδ T cell therapies by TC BioPharm and Gadeta, and TCR-NK approaches by Syena.
Innovations in targets, technologies, and strategic models continue to shape the unique value of TCR-focused companies. Related approaches, including tumor infiltrating lymphocytes, antigen specific T cells, and TCR engineered T cells, are also being evaluated to fight cancer more effectively. Together, these efforts expand the broader landscape of T cell therapies for solid tumors, with ongoing work to maintain specificity for tumor cells and reduce risk to healthy cells.
KACTUS Solutions for TCR Therapy Development
To support TCR therapy developments, KACTUS has established a comprehensive portfolio of services, offering custom expression services for TCRs, TCR-related biologics, and MHC-peptide complexes. These solutions are designed to accelerate drug development for companies working in the TCR therapeutic space. This supports engineered cell therapy programs and broader T cell therapies intended to transform cancer care by enabling precise antigen recognition.
Our team has successfully expressed Tebentafusp, demonstrating its ability to bind both the GP100 (HLA-A*02:01) complex and the CD3 heterodimer—exhibiting robust dual-binding activity. In development workflows, functional screening can include assessing activity across cell clones and confirming that engineered constructs behave consistently in relevant assay systems.
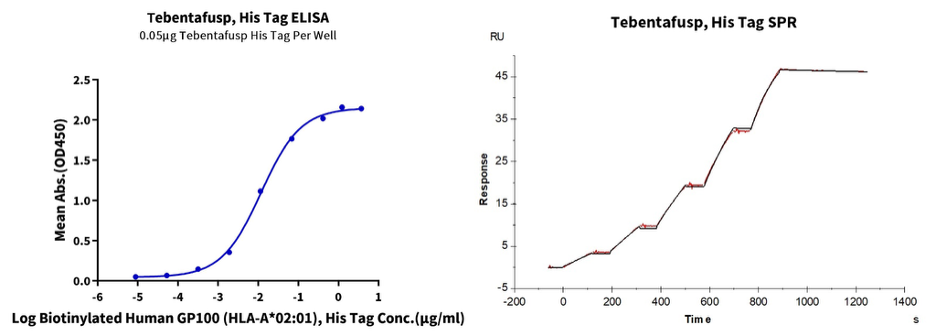
Figure 5. In ELISA (left) and SPR (right) analyses, Tebentafusp binds to both the monomeric and tetrameric forms of the Human GP100 (HLA-A*02:01) complex, with an EC₅₀ of 11.8 ng/mL and an affinity constant (Kᴅ) of 0.196 nM. Such datasets help validate that the therapy engages the intended tumor antigens while enhancing efficacy.
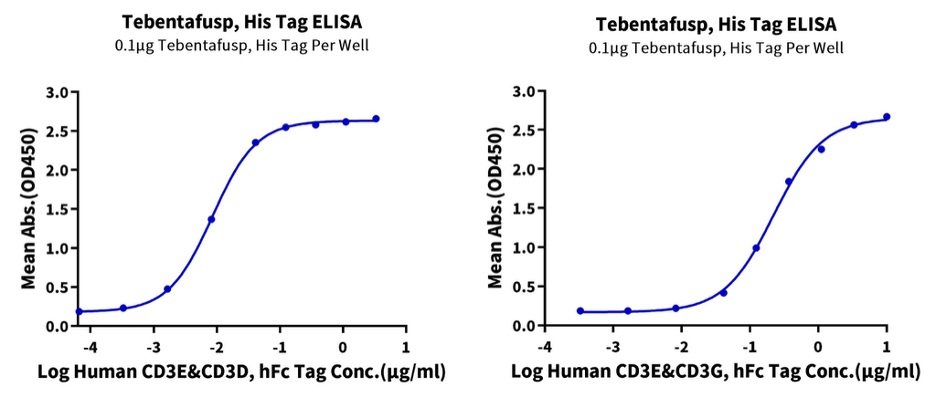
Figure 6. ELISA results confirm that Tebentafusp binds to both CD3E&CD3D and CD3E&CD3G heterodimers, with EC₅₀ values of 8.7 ng/mL and 0.22 μg/mL, respectively. These readouts support selection of candidates designed to destroy cancer cells while limiting activation against healthy cells.
In addition, KACTUS MHC-peptide complex products exhibit excellent biological activity, making them ideal for use in immunization or screening studies within TCR therapy development—helping researchers identify the correct molecular sequences.’This can include confirming presentation of target antigens derived from intracellular proteins and assessing risk of cross reactivity across normal cells.
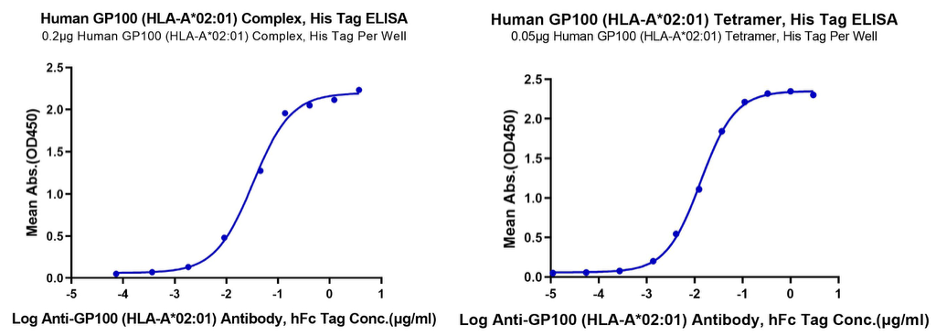
Figure 7. ELISA results demonstrate that both the monomeric and tetrameric forms of Human GP100 (HLA-A02:01) can bind to the Anti-GP100 (HLA-A02:01) antibody, with EC₅₀ values of 32.9 ng/mL and 28.3 ng/mL, respectively.
TCR & MHC Products, Services, & Resources
● MHC & TCR Solutions | Brochure
● TCR Detection Using Peptide-Ready MHCs | Case Study
● Engineering MHC Reagents | Poster
● Surfact Plasmon Resonance (SPR) Services | Brochure
For more information, please contact us at support@kactusbio.us. (For readers comparing modalities: CAR-T cell therapy is widely used in certain blood cancers and often manufactured from cells collected from a patient’s bloodstream, while TCR-T focuses on tumor antigens presented by MHC molecules—expanding options for solid tumors.)
References
-
Natarajan K, Jiang J, May NA, Mage MG, Boyd LF, McShan AC, Sgourakis NG, Bax A, Margulies DH. The Role of Molecular Flexibility in Antigen Presentation and T Cell Receptor-Mediated Signaling. Front Immunol. 2018 Jul 17;9:1657.
-
Tsimberidou AM, Van Morris K, Vo HH, Eck S, Lin YF, Rivas JM, Andersson BS. T-cell receptor-based therapy: an innovative therapeutic approach for solid tumors. J Hematol Oncol. 2021 Jun 30;14(1):102.
-
Chandran SS, Klebanoff CA. T cell receptor-based cancer immunotherapy: Emerging efficacy and pathways of resistance. Immunol Rev. 2019 Jul;290(1):127-147.

60 Hickory Drive
Waltham, MA 02451
United States